
Home Boris Sidis Archives Menu Table of Contents Next Chapter
|
THE PSYCHOLOGY OF SUGGESTION Boris Sidis, Ph.D. © 1898. New York, D. Appleton and Company. |
CHAPTER XXIII
FORMS OF SUBCONSCIOUS STATES AND TYPES OF AMNESIA
WITH the case of H. before us, we return once more to the discussion of subconscious states and types of amnesia. In our analysis of consciousness we arrived at the conclusion that consciousness consists of momentsconsciousness. A moment-consciousness contains as much psychic matter or moments-content as is present within one given synthesis of consciousness. Now, the subconscious includes within it the sum total of all the moments-content and also of an the moments-consciousness in a condition of indifferent association and dissociation.
The subconscious is not a selective activity; it simply stands for the sum total of all the moments-consciousness. In the moment-consciousness, again, selection is absent; it is simply a matter of chance what psychic matter shall enter into the synthesis of the momentconsciousness. It is only as we reach the higher plane of psychic life characteristic of the primary self, it is only then that we for the first time meet with selective activity. The primary self, being an active self-conscious synthesis, is selective in its nature. Out of a number of sensations, ideas, and feelings the activity of the primary self selects only some, and leaves the rest in the background of consciousness. The primary self has its more or less definite, determinate outlines that constitute its personal character. Only material of a certain kind and quality, only moments-content and moments-consciousness of a definite character fitting into the form activity of the self, only such material is taken up within the circle of its experience; the rest of the material is simply ignored. This leaving out, this ignoring of many moments, ranges through all degrees of synthetic activity, from the laying up of the moments with a view to further use, from the possibility of synthetizing the rejected material up to the total ignoring of it, when the material is entirely resigned, never to be used again because of its total incongruence with the character of the selective activity or because of the weakness within the energy of the synthetic agency. Many mental diseases, and especially those that go under the collective name of hysteria, have as their psychic cause some of those conditions or all of them in different combination and in various degrees of intensity.
This ignoring of mental material, ranging through all shades and degrees, and also the selective synthetic agency, having different degrees of weakness in the energy of its intensive and extensive activity, give rise to dissociation of mental states, to disaggregation of synthetized moments from those that were not taken up in that particular synthesis that constitutes for the time being the patient's principal individuality. All the types and degrees of amnesia depend on the nature and degree of such dissociation or disintegration. Where the dissociation is incomplete the amnesia will also be incomplete.
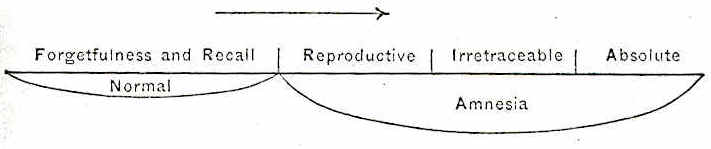
Moments-consciousness as well as moments-content may drop out from the unity of the synthetic consciousness and produce forgetfulness or amnesia. In such a kind of amnesia, however, the gap formed is felt and appreciated by consciousness as a gap. Glimpses of memory come back and disappear again; the forgotten moments tend to recur time and again. The range of such an amnesia varies greatly, from simple forgetfulness of some few details to the oblivion of many important events. This type of amnesia may be characterized as reproductive or recurrent.
Where the dissociation, however, is complete, the amnesia in regard to the disaggregated new synthetized material is total. Under conditions that bring about a disruption in consciousness the whole moment of synthetic self-consciousness may in a disaggregated form fall into the region of desultory moments-consciousness, and very frequently with a tendency to combine and emerge at the first favorable opportunity to the surface of the primary consciousness. Meanwhile, another series of moments-content and of moments-consciousness rise to the level of the upper consciousness and become synthetized in another different moment that takes the place of the disaggregated one. Between the two moments there is a break, a gap; fragmentary reproduction of the one by the other is not impossible; if induced by certain methods, the recognition element may be present, but may also be totally lacking. This form of amnesia may be termed irretraceable.
Many of the former moments consciousness and moments content may come up in this newly formed moment consciousness, still the moment, on the whole, is new and different synthesis. Hence we may say that irretraceable amnesia is the possible manifestation of the phenomena of double consciousness.
We may put it down as a law, that the degree of amnesia is proportional to the amount of psychophysiological disaggregation.
The psycho-physiological process of dissolution may extend still further and deeper. From a disaggregation of systems of moments-consciousness the process may pass into a disintegration of the moments-content themselves, and the amnesia then is absolute; for a disintegration of the moment content itself practically means a total loss of that psychic content and the impossibility of its reinstatement in the synthesis of moment consciousness.
The physiological side of amnesia is to be found in the disaggregation of clusters of cells into their constituent systems and groups. This disaggregation is due to the violent, hurtful impressions of strong stimuli that effect a contraction of these systems and groups joined by association fibres into clusters. Under the influence of some strong injurious stimulus a whole system or group may withdraw from a constellation of co-ordinate systems of cells, but in such a way that the contraction is effected only in relation to some of the systems―that is, only some of the association paths get interrupted, while through other paths the system still stands in connection with the cluster or constellation. There will, of course, be amnesia, but it will be of a vacillating, unstable character, because the connection of the disaggregated system can be effected in an indirect way through other systems. Such amnesia will be reproductive. The easiness with which this reproduction can be brought about is in inverse proportion to the extent of disaggregation effected, in inverse proportion to the number of interrupted association paths.
If, however, the system has contracted completely, and has fully withdrawn from the cluster of systems so that all association paths are interrupted, the result is complete irretraceable amnesia.
In irretraceable amnesia the system that has withdrawn is perfectly sound, only it possesses groups of cells of a less complex nature, and the former connections can be again reinstated under favorable circumstances. Should, however, the hurtful stimulus be of such a nature as to destroy a whole system of cells, then the amnesia effected is absolute. The connections can not any more be reinstated, because the system itself is destroyed.
The process of disaggregation setting in under the action of strong and hurtful stimuli is not something new and different in kind from the usual; it is a continuation of the process of association and dissociation normally going on in the higher constellations. The one process gradually passes into the other with the increase of the intensity or duration of the hurtful stimulus. Both processes are of one and the same nature. A further continuation of the process of disaggregation passes into that of cell destruction, which, accepting Dr. Ira Van Gieson's terminology of cell disintegration, may be characterized as cytoclasis1
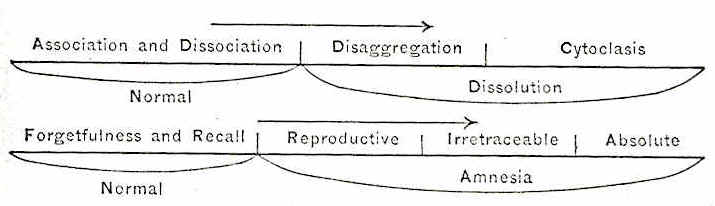
The process may be represented as follows:
Psychologically, we find that different degrees of amnesia shade into each other imperceptibly, and that between the two extremes―namely, that of normal forgetfulness and that of absolute amnesia―there exists a whole uninterrupted series of gradations of amnesia, forming a continuous progression.
This may graphically be represented as follows:
We may now no co-ordinate the two series and graphically represent them by two parallel lines.2
In reproductive or recurrent amnesia the patient must make a special effort to bring out the dissociated experiences, and the strength of the effort is proportional to the amount of dissociation. In irretraceable amnesia the patient can by no effort of will bring back the lost memories, but they emerge under artificial conditions, such as in the state of hypnosis or in the induction of slight hypnoidal states, when isolated ideas and sensations, fragments of experiences, without being recognised as past, emerge to the surface of consciousness; also in hypnoidic states, when all the memories are found to be present. The case of Hanna is a fair example. In the hypnoidic states, as the "vision dreams," the patient proved to know everything he had forgotten in his seemingly normal waking state.
In absolute amnesia, however, there are no means by which the lost memories may be restored; no psychic condition can reinstate them in consciousness. They are gone and lost, never to return; they are utterly destroyed.
From a practical clinical standpoint it is of vital importance to make a differential diagnosis as to the kind of amnesia. In a case of amnesia with no possibility on the side of the patient, no matter how strong the efforts are, to bring up the lost memories, it is of the utmost importance to find out whether it is a case of irretraceable or a case of absolute amnesia, as the prognosis and treatment in each one of the two maladies are totally different. To make such a diagnosis, the subconscious must be tapped by means of different methods.
The clinician, the alienist, must bear in mind that a case of amnesia, where the lost memories lie beyond the control of the patient, may be irretraceable, disaggregative, and therefore curable, or absolute, cytoclastic, and therefore completely incurable.
Turning now to irretraceable or disaggregative amnesia, we find that hypnotic, hypnoid3, hypnoidic, and hypnoidal states reveal the presence of lost memories in the depths of the subconscious self. Memories which the upper personality is unable to recall, and which seem to be altogether obliterated, suddenly' emerge to the surface of consciousness with the removal of the upper layers of mental activity. In hypnosis the removal of the waking consciousness is followed by a state of high reflex suggestibility characteristic of the indefinite nature of the secondary self. In the hypnoidic state such suggestibility is absent, because another quasi-personality emerges with a more or less definite character, a personality that is inaccessible to direct suggestion. The hypnoidic state, however, is amenable to indirect suggestion. By means of indirect suggestion it is even possible entirely to remove this hypnoidic personality, and have it replaced by another one, which in its turn may be treated in ike manner.
The character of the hypnoidic individuality is some outlived phase of the patient's personal life. Such states may also be induced in hypnosis, but then the hypnoidic state is vague and ill defined. More frequently the hypnoidic state may be fully brought about in post-hypnotic or what may be termed hypnonergic states. I could effect such an analogous state in my somnambulic subjects by post-hypnotic suggestion. The difference between the post-hypnotic or hypnonergic and the true spontaneous hypnoidic state consists in the relation of the subject to external impressions. In the hypnonergic state the subject receives external impressions directly and refers them to some external source. He hears, sees, feels, perceives things that happen around him, and frequently carries on very animated conversations on different topics. Even in the case of post-hypnotic negative hallucinations, the patient is still fully alive to other not inhibited sense impressions that reach him from all sides. Quite different is the true hypnoidic state. The sense organs of the patient are closed to the impressions of external stimuli. He does not perceive anything that takes place around him. His environment is that of the past, and in it he lives and moves. Shut up within one of his past lives, he remains insensible to the world of his objective present. If by chance any impressions do reach the subject, they are at once worked into his present hallucinatory life experience. If the patient is touched, squeezed, pricked, he feels nothing at all; he is totally anæsthesic and analgesic, and still within his "vision" he may be extremely sensitive to pain, shiver from cold, complain of fatigue, and tortures of pricking sensations caused by a strong gale blowing icicles into his face. Of such a nature were the visions in the case of Hanna.
The patient hears none of the conversation carried on in his presence. When the patient is spoken to on subjects not directly related to his resurrected life experience, he makes no reply; he simply does not hear. Only when he is addressed on something relating to the experience he is passing through, it is only then that he makes a reply. He does not realize, however, that it is some one else who speaks to him; his replies to questions are to him either answers to his own thoughts, or sometimes―a case very rare―he seems to converse with some imaginary person within his hypnoidic state.
No suggestions are taken by the hypnoidic personality. It is fully rational in relation to the environment in which it lives. Thus, in one of his hypnoidic states Rev. Thomas C. Hanna lived through a terrible accident that happened to him once. He was on Mount Jewett, Pa. The wind blew high. Lightning rent the sky, thunder crashed overhead. The gale gained strength and became a tempest. Broken branches and trees were falling on all sides. "There is an old woman with a child!" he exclaimed. "Oh, it is terrible! it is terrible!" he moaned. "We must run! We must run! I must drag the woman. Thunder! It is terrible! Save the woman! I am so cold! My heart is so weak! Oh, it is terrible! We must run! we must run!" To my question whether he knew Miss C., the answer of the hypnoidic personality was highly interesting" and instructive. "Don't know her yet―acquainted with her a year later. From Mount Jewett to her is a year." (This was found to be correct.) When I suggested to him that his friend S. was with him, he laughed me to scorn. "That is impossible!" he exclaimed; "S. is many miles away from here." I asked for the date. He gave the date in which the event took place. "It is August now," he said. When I insisted that it was May (the actual time when the vision occurred), the hypnoidic personality became impatient, raised its hand, struck the bed with great force, and exclaimed: "I am sure it is now August. You can not make me crazy! "
All the time the patient was sitting up in his bed, with his eyes firmly shut, blind and deaf to all impressions that had no relation to the "vision." By indirect leading questions this particular personality gradually dwindled away, and lo! a new personality appeared on the scene―a boy personality.
The Rev. Thomas C. Hanna became a boy of thirteen. The scenery changed completely. He was on Umbrella Island. It was sunset, it was "beautiful." He was expected for supper, but he was on the water, rowing and fishing.
On awakening from his hypnoidic state the patient remembered the "vision" very clearly; he could reproduce it, as if it were impressed on his mind in images of fire. He could not recognise the experiences of his vision as events that had taken place in his past life; he did not know that I or anyone else conversed with him and led him to give answers; nor did he remember any of the many statements to my indirect questioning he had made in his hypnoidic state. He could not remember the answers he gave me on the suggestion that his friend S. was with him; he did not know anything of the quarrel we had about the date; nor did he remember anything of the interesting information he gave me about the events of his life, such as the date of his acquaintance with Miss O. He could only remember, and that with extraordinary clearness and distinctness, everything that directly related to the "vision" itself.
Left to itself the hypnoidic personality tends to disappear, to fall back into the undifferentiated mass of moments-consciousness of the subconscious self, for the hypnoidic personality is unstable in its nature. Unstable, however, as the hypnoidic personality is, it is in closer contact with the subconscious life than is the waking self. The hypnoidic personality is in possession of facts, experiences, memories, of which the upper central consciousness is entirely ignorant. Absolute amnesia, where there is full destruction of psychic experience, is the only type of amnesia that may touch the hypnoidic personality; all other forms of amnesia are maladies of the upper self.
The hypnoidal states are of an entirely different nature. They are sudden intrusions of isolated momentsconsciousness into the upper regions of the waking personality, and can be induced by post-hypnotic suggestion, as well as by methods of hypnoidization. Like the hypnoidic, the hypnoidal states are outlived experiences, but, unlike the hypnoidic state, they are not outlived personalities. The hypnoidal states are bits, mere fragments of past experiences.
In hypnoidal states past, outlived experiences heave up into the upper consciousness from the depths of the subject's subconscious life. The subject does not welcome these experiences as his own; he does not recognise them as belonging to the stream of his conscious life once lived through; they are volcanic eruptions from the subconscious life.
The hypnoidal differ from the hypnoidic states in four very important points:
1. They can be and usually are artificially induced by the method of hypnoidization. The hypnoidic can not be artificially induced; they are always spontaneous.
2. The upper consciousness takes direct cognizance of the hypnoidal states in the moment of their appearance. The hypnoidic states are not directly cognized by the upper consciousness; the latter is always absent when the hypnoidic states are present.
3. The experience of hypnoidal states is vague, and tends to disappear from the upper consciousness the next moment after its occurrence. The experience of the hypnoidic state is inscribed on the mnemonic tables of the upper consciousness in letters of fire.
4. While the hypnoidic states form complete systems of experiences, whole personalities, the hypnoidal states are mere bits, chips of past experiences.
In both states, hypnoidic and hypnoidal, we find, however, one common trait, and that is the emergence of moments-consciousness that may be known and recalled, whether directly or indirectly, by the primary self. These experiences, as we pointed out, are not remembered as past; they are not regarded as experiences that had taken place within the former life history of the patient.
The most important element of memory―namely, recognition―is here totally absent; for memory is the reproduction and recognition of one's past conscious experience. Hence, where this recognition element is lacking, there true memory is also absent. The reproduction of past experience without the element of recognition, a condition of mind characteristic of hypnoidic and hypnoidal states in their relations to the upper consciousness, may be termed recognitive amnesia.
In contradistinction to this type of amnesia, there is another one where not only recognition but even the synthesis of reproduction is absent. Such a type may be termed synthetic amnesia.
lrretraceable amnesia may be recognitive or synthetic.
The dissociated moment may come and go, may suddenly emerge, to the surprise of the patient, to the upper stream of consciousness, be synthetized, sometimes even recognised, and then be lost again. Such a lapse of memory may be termed simple amnesia.
Where the loss of memory is for events of a certain period, as an hour, a day, a month, or even several years, and where all events before and after that gap can be recalled, then we have that type of amnesia which is characterized as localized amnesia.
If the loss of memory is only for certain systems of events, while other events that happened at the same time can be fully recalled, such a loss is termed systematized amnesia.
When the lost content remains unaltered during the whole course of the disease, the amnesia is stable.
If the amnesia sets on at intervals, it is periodic.
If psychic states keep on alternating, each one being completely amnesic for the other, such as is the case in double-consciousness, then the amnesia is alternating.
When the content of memory is continually decreasing, ending at last in a more or less total loss of it, such as we find in general paralysis, then the amnesia is progressive.
The dissociation in consciousness may he in relation to sensations. The patient experiences the sensation but does not comprehend its meaning. This may he termed sensory or perceptual amnesia. This form of amnesia may be limited to one or two classes of sensations, or may extend to all of them.
If the amnesia is of one sense, it may be called local; if of all of them, total sensory amnesia.
Where the dissociation occurs in the motor consciousness or motor centres, the amnesia is motor. This type may he again local or total.
If the amnesia is of the whole life experience, as it is in the case of Rev. H., it may he termed general.
If, however, the amnesia is of but a part of life experience, as, for instance, in cases of aphasia, or of localized amnesia, it may he termed special.
If the cause of the amnesic state is some intense mechanical stimulus, such as a fall or a blow on the head, the amnesia is traumatic.
Amnesia is toxic when the cause is some extrinsic poison absorbed by the organism, as, for instance, in the case of alcoholic intoxication.
Amnesia is autotoxic when the poison that causes the disease is periodically developed by the organism itself, on account of its defective working and imperfect elimination of waste products. Such cases of amnesia may occur in the status epilepticus, in the states of mind that go under the name of psychic equivalent of epilepsy, which are found interspersed in the series of typical epileptic motor attacks that are accompanied by a mental activity that can rise no higher than the most elementary desultory moment-consciousness.
If amnesia is the result of fatigue, of nervous exhaustion, or of the instability of central organization, it may be termed asthenic.
Amnesia is emotional or pathematic when the cause of it is an intense emotion.
These types of amnesia occur spontaneously in many mental diseases, and can also be produced artificially by hypnotic suggestion. Whether artificial or spontaneous, the mechanism of these types is at bottom the same―it is a disaggregation or disintegration of moments-consciousness.
Thus there are three types of amnesia, if regarded from the standpoint of extensiveness:
1. Reproductive.
2. Irretraceable or disaggregative.
3. Absolute or cytoclastic.
According to intensiveness, there are three types of amnesia:
1. Simple.
2. Recognitive.
3. Synthetic.
According to the lost content, amnesia has six types:
1. General.
2. Special.
3. Localized.
4. Systematized.
5. Sensory, local or total
6. Motor, local or total.
According to stability or fluctuation of content amnesia has four types:
1. Stable.
2. Periodic.
3. Alternating.
4. Progressive.
Etiologically, or according to cause, there are five types of amnesia:
1. Traumatic.
2. Toxic.
3. Autotoxic.
4. Asthenic.
5. Emotional or pathematic.
A summary of all the principal forms of subconscious states and of all the types of amnesia gives the following table:
Forms of subconscious states:
1. Hypnotic.
2. Somnambulic.
3. Hypnonergic.
4. Hypnoid.
5. Hypnoidic.
6. Hypnoidal.
7. Hypnoleptic.
Types of amnesia:
1. Reproductive or recurrent.
2. Irretraceable or disaggregative.
3. Absolute or cytoclastic.
4. Simple.
5. Recognitive.
6. Synthetic.
7. Localized.
8. Systematized.
9. Sensory, local or total.
10. Motor, local or total.
11. General.
12. Special.
13. Stable.
14. Periodic.
15. Alternating.
16. Progressive.
17. Traumatic.
18. Toxic.
19. Autotoxic.
20. Asthenic.
21. Emotional or pathematic.
________________
1. See Dr. Van
Gieson's article, The Toxic Basis of Neural Diseases, State Hospitals' Bulletin,
No. 4.
2. The physiological process of association and dissociation
corresponds to the psychological process of forgetfulness and recall; the
process or disaggregation, to the forms of reproductive and irretraceable
amnesia. Cytoclasis is concomitant with absolute amnesia.
3. By the term "hypnoid" I indicate the coexistence of two
or more fully independent functioning constellations of moments-consciousness
such as is presented in the phenomena of automatic writing and of hysteria. An
experimental study of cases of hypnoid states and the method of their complete
and permanent cure will appear in The State Hospitals' Bulletin.
![]()